Rectal Cancer
What is a Rectal cancer?
Rectal cancer is cancer that begins in the rectum. The rectum is the last several inches of the large intestine. It starts at the end of the final segment of your colon and ends when it reaches the short, narrow passage leading to the anus.
Cancer inside the rectum (rectal cancer) and cancer inside the colon (colon cancer) are often referred to together as “colorectal cancer.”
Symptoms
Signs and symptoms of rectal cancer include:
- A change in bowel habits, such as diarrhea, constipation or more-frequent bowel movements
- Dark maroon or bright red blood in stool
- Narrow stool
- A feeling that your bowel doesn’t empty completely
- Abdominal pain
- Unexplained weight loss
- Weakness or fatigue
Causes
Rectal cancer begins when healthy cells in the rectum develop changes (mutations) in their DNA. A cell’s DNA contains the instructions that tell a cell what to do.
The changes tell the cells to grow uncontrollably and to continue living after healthy cells would die. The accumulating cells can form a tumor. With time, the cancer cells can grow to invade and destroy healthy tissue nearby. And cancerous cells can break away and travel (metastasize) to other parts of the body.
For most rectal cancers, it’s not clear what causes the mutations that cause the cancer to form.
Risk factors
Factors that may increase the risk of rectal cancer are the same as those that increase the risk of colon cancer. Colorectal cancer risk factors include:
- Older age. Colorectal cancer can be diagnosed at any age, but most people with this type of cancer are older than 50. The rates of colorectal cancer in people younger than 50 have been increasing, but doctors aren’t sure why.
- African-American descent. People of African ancestry born in the United States have a greater risk of colorectal cancer than do people of European ancestry.
- A personal history of colorectal cancer or polyps. Your risk of colorectal cancer is higher if you’ve already had rectal cancer, colon cancer or adenomatous polyps.
- Inflammatory bowel disease. Chronic inflammatory diseases of the colon and rectum, such as ulcerative colitis and Crohn’s disease, increase your risk of colorectal cancer.
- Inherited syndromes that increase rectal cancer risk. Genetic syndromes passed through generations of your family can increase your risk of colon and rectal cancer, including FAP and Lynch syndrome.
- Family history of colorectal cancer. You’re more likely to develop colorectal cancer if you have a parent, sibling or child with colon or rectal cancer.
- Eating a diet low in vegetables. Colorectal cancer may be associated with a diet low in vegetables and high in red meat, particularly when the meat is charred or well done.
- Too little exercise. If you’re inactive, you’re more likely to develop colorectal cancer. Getting regular physical activity may reduce your risk of cancer.
- Diabetes. People with poorly controlled type 2 diabetes may have an increased risk of colorectal cancer.
- Obesity. Obese people have an increased risk of colorectal cancer when compared with people considered at a healthy weight.
- Smoking. People who smoke may have an increased risk of colorectal cancer.
- Drinking alcohol. Regularly drinking more than three alcoholic beverages a week may increase your risk of colorectal cancer.
- Radiation therapy for previous cancer. Radiation therapy directed at the abdomen to treat previous cancers may increase the risk of colorectal cancer.
Prevention
To reduce your risk of colorectal cancer, consider trying to:
Talk to your doctor about cancer screening. Colorectal cancer screening reduces the risk of cancer by identifying precancerous polyps in the colon and rectum that could develop into cancer. Ask your doctor when you should begin screening. Most medical organizations recommend starting screening around age 50, or earlier if you have risk factors for colorectal cancer.
Several screening options exist — each with its own benefits and drawbacks. Talk about your options with your doctor, and together you can decide which tests are appropriate for you.
- Exercise most days of the week. Try to get at least 30 minutes of exercise on most days. If you’ve been inactive, start slowly and build up gradually to 30 minutes. Also, talk to your doctor before beginning any exercise program.
- Eat a variety of fruits, vegetables and whole grains. Fruits, vegetables and whole grains contain vitamins, minerals, fiber and antioxidants, which may play a role in cancer prevention. Choose a variety of fruits and vegetables so that you get an array of vitamins and nutrients.
- Maintain a healthy weight. If you’re at a healthy weight, maintain it by exercising regularly and choosing a healthy diet. If you’re overweight, work to lose weight slowly by increasing exercise and reducing the number of calories you eat.
- Stop smoking. If you smoke, stop. If you’re having trouble quitting, talk to your doctor about options. Medications and counseling may help.
- Drink alcohol in moderation, if at all. If you choose to drink alcohol, do so in moderation. For healthy adults, that means up to one drink a day for women and up to two drinks a day for men.
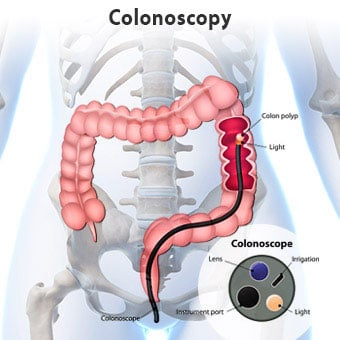
What actually happens in Colonoscopy?
With you resting on your left side, your doctor will gently examine your back passage with a gloved
finger & lubricating jelly before carefully inserting the colonoscope. Air is then usually passed through
the tube into the colon to make it expand and the bowel wall easier to see. This may briefly cause pains
similar to having wind and you may get an urge to go to the toilet, but as the colon is empty, this won’t
be possible.
Most people pass some wind. There is no need to feel embarrassed about this as your doctor will expect
this to happen. During the procedure, you may be asked to change your position – for example turning
from your side onto your back. This helps your doctor to examine different areas of the colon more
easily. If necessary, your doctor will take a biopsy and/or remove polyps. This is done using special
instruments passed inside the colonoscope, and is quick and painless.
I would prefer sedation for the procedure!
Our Anaesthesia team will make sure you are comfortable throughout the procedure. It would be
preferable for them to review your records in advance, so they can plan appropriately for the day of the
procedure. The sedative will be injected through the cannula placed in the back of your hand, and you
should start to feel relaxed and drowsy almost immediately. Sedatives can sometimes affect your
breathing, so the amount of oxygen in your blood will be monitored constantly through a clasp on your
finger and you may be given extra oxygen through a mask.
After your procedure is complete you will be taken to the recovery area. The nurses there will continue
to monitor your blood pressure, pulse and oxygen saturation. Your “significant other” or friend may
come sit with you in recovery at this time. You may need to stay in the recovery area for even up to
three hours. Plan so you do not need to drive, operate machinery, sign any important documents or
make important decisions until the next day. You should not exercise strenuously until the next day.
You must make arrangements for a responsible adult to drive you home after your procedure. Taxis and
buses are not permitted unless you are accompanied by a responsible adult.